The abducens (CN VI) nucleus is located in the caudal part of the pons. It lies just under the floor of the fourth ventricle, medial to the sulcus limitans.

The nucleus contains two main groups of neurons: motor neurons and interneurons. It contains also a third group, a small number of neurons that send their axons to the flocculus of the cerebellum.
Motor neurons of the abducens nucleus form the ipsilateral abducens nerve (the sixth cranial nerve, CN VI). Abducens nerve is a pure motor nerve and innervates the lateral rectus muscle of the ipsilateral eye. The main function of the muscle is to abduct the eye.
Axons of the interneurons of the abducens nucleus enter medial longitudinal fasciculus (MLF), cross to the contralateral side and travel as the contralateral MLF rostrally to the oculomotor nucleus. (Interneurons from the left abducens nucleus travel most of their way through the right MLF and vice versa.) Interneurons project to the part of the contralateral oculomotor nerve nucleus that contains motor nerve bodies for the medial rectus muscle. This kind of arrangement of connections between abducens and oculomotor nuclei and nerves allows for conjugate horizontal eye movements.
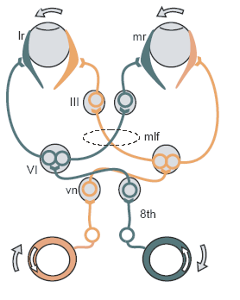
A lesion of the interneurons, for example in the medial longitudinal fasciculus, causes failure of conjugate eye movements manifested by the paralysis of adduction of the contralateral eye. With an attempt to look to the side of the eye ipsilateral to the damage of the MLF the ipsilateral eye abducts with nystagmus and contralateral eye stays in the middle. The condition is known as internuclear ophthalmoplegia (INO). There is nothing wrong with the medial rectus muscle or the oculomotor nerve of the contralateral eye in this condition. That same contralateral eye that cannot adduct during the conjugate gaze, often can adduct during the convergence of the eyes.
Damage to the abducens nerve that occurs after the separation of the axons of the interneurons causes isolated paralysis of abduction of the ipsilateral eye.
Unilateral damage to the abducens nucleus causes lateral gaze paralysis, i.e. a binocular gaze paralysis in the direction of the lesion because both the motoneurons and interneurons in the nucleus are damaged.
The abducens nucleus is supplied by the pontine branches of the basilar artery.
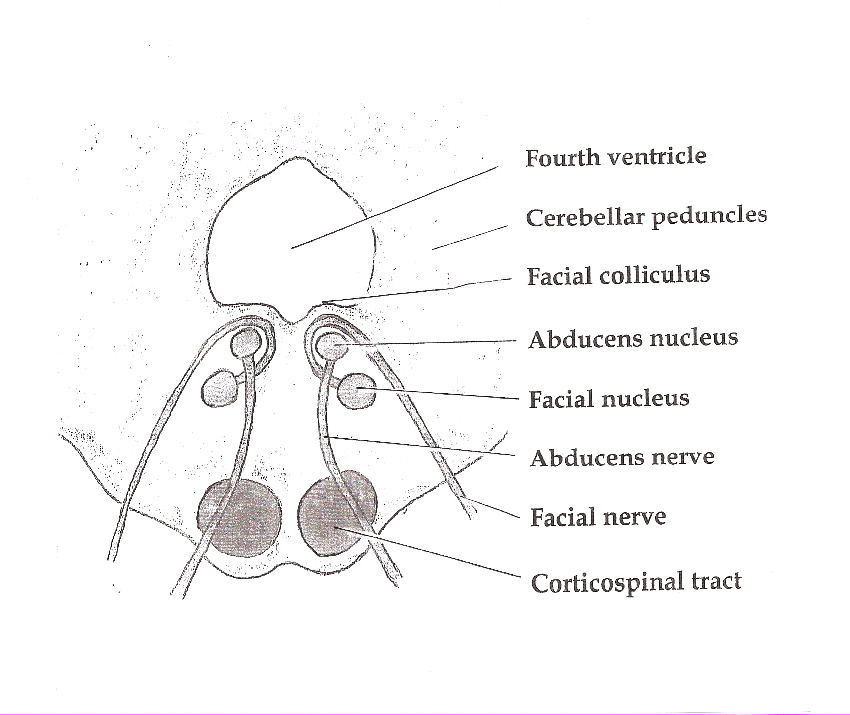
Facial colliculus
Motor fibers of the facial nerve, originating from the facial motor nucleus, loop around the ipsilateral abducens nucleus. Together they form the facial colliculus . Because the fibers of the facial nerve and the abducens nucleus are positioned so close to each other, infarcts and other lesions that occur in the dorsal caudal pons can cause both the ipsilateral lateral gaze palsy and the ipsilateral facial palsy.
The facial motor nucleus is situated deeper in the tegmentum of the pons. It is supplied by the labyrinthine arteries, which are branches of the anterior inferior cerebral artery (AICA).
Clinical syndromes
Möbius syndrome is a congenital disorder characterized by hypoplasia or atrophy of cranial nerve nuclei. Abducens and facial nerves are involved in most of the cases, which causes facial and abducens paresis. Facial paresis is most often bilateral. Bilateral abducens hypoplasia/atrophy causes complete horizontal gaze paresis.
One-and-a-half syndrome is caused by an ipsilateral damage of both the MLF and abducens nucleus. Let us say that the damage happened on the right side. Because of the damage to the MLF, the right eye cannot adduct with an attempt of a lateral gaze. The left eye cannot adduct with an attempt to the gaze to the right because interneurons in the right abducens nucleus are damaged. The right eye cannot abduct because the right abducens nucleus is damaged, that one is easy. The only thing that can happen with an attempt to a horizontal gaze is abduction of the left eye, often with a nystagmus.
To put it another way, an unilateral lesion of the MLF and abducens nucleus causes lateral gaze palsy in the direction of the lesion and internuclear ophthalmoplegia.
Eight-and-a-half syndrome is one-and-a-half syndrome plus ipsilateral peripheral facial palsy. Ipsilateral to the side of the lesion or clinically, to the side of the eye that cannot abduct.
Millard–Gubler syndrome is an example of a clinical syndrome caused by a lesion in the caudal pons which causes damage to both the facial and abducens nerve, but not to the abducens nucleus. The lesion is located in the ventral portion of the caudal pons. It affects fascicles of abducens and facial nerve and uncrossed fibers of the corticospinal tract.
The syndrome is manifested with ipsilateral peripheral facial paralysis, contralateral hemiparesis/hemiplegia in the arms and legs, and ipsilateral weakness of the abduction of the eye. There is no binocular gaze paresis because the abducens nucleus is not damaged.
OSMCQs
References:
Somani AN, Adesina O. Neuroanatomy, Abducens Nucleus. [Updated 2021 Oct 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544265/
Yoo H, Mihaila DM. Neuroanatomy, Facial Colliculus. [Updated 2021 Oct 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555907/
Sakuru R, Elnahry AG, Bollu PC. Millard Gubler Syndrome. [Updated 2022 Feb 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532907/